Developmental Dysplasia of the Hip (DDH) is a condition where the hip joint does not develop properly in infants and young children. It ranges from mild instability to complete dislocation of the femoral head from the acetabulum. Early diagnosis and treatment are crucial to ensure normal hip development and to prevent long-term complications such as pain, limping, and early osteoarthritis.
When non-surgical methods such as bracing or closed reduction fail or are not feasible, surgical intervention becomes necessary. Open reduction is a key surgical procedure used to treat DDH, especially in older infants and children where the hip joint cannot be reduced by closed methods.
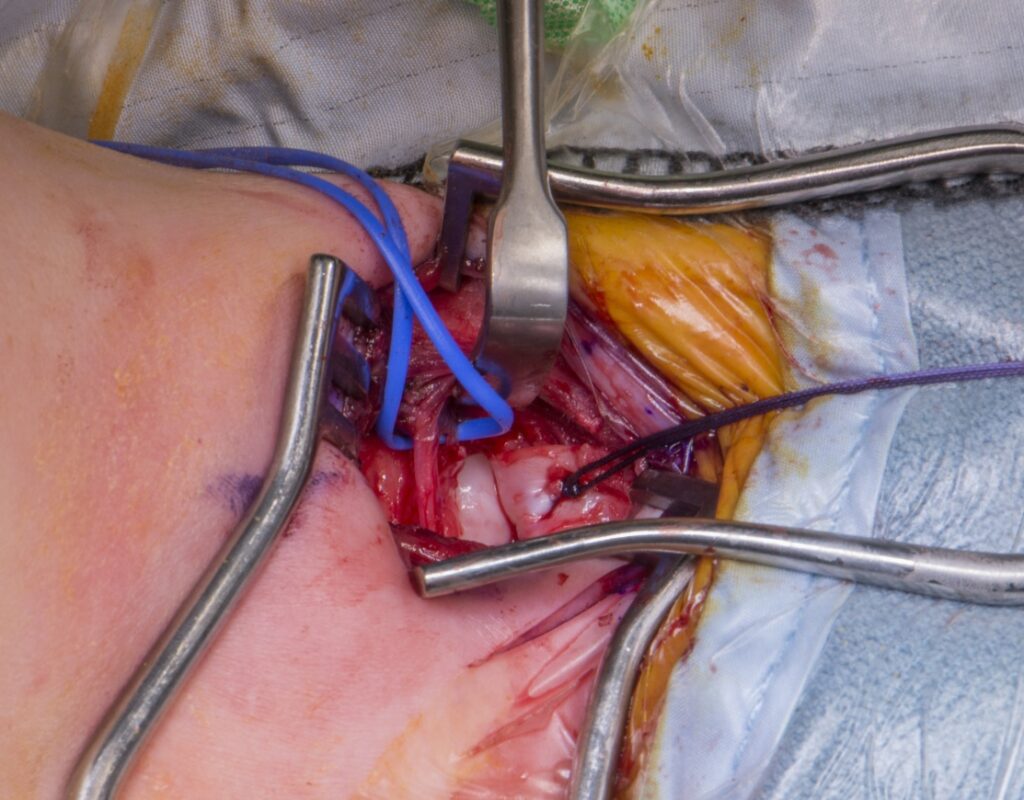
Open reduction is a surgical technique that involves making an incision to directly visualize and manipulate the hip joint to relocate the femoral head into the acetabulum. Unlike closed reduction, which is performed without an incision using traction and manipulation under anesthesia, open reduction allows the surgeon to remove obstacles preventing proper hip alignment and to repair soft tissues.
Open reduction is typically indicated in the following scenarios:
Before surgery, a thorough clinical and radiological assessment is essential. This includes:
Open reduction is performed under general anesthesia. The child is positioned supine or lateral depending on the surgical approach.
Several approaches exist, with the most common being:
After surgery, the child is immobilized in a spica cast for 6 to 12 weeks to maintain reduction and allow healing. Pain management, monitoring for complications, and regular follow-up with imaging are essential.
Physical therapy is introduced gradually after cast removal to restore hip motion and strength.
Open reduction for DDH has a high success rate in achieving stable, concentric reduction of the hip joint. Early intervention generally leads to better outcomes. However, the prognosis depends on factors such as:
Potential complications include avascular necrosis of the femoral head, redislocation, stiffness, and residual dysplasia.
As with any surgery, open reduction carries risks:
Open reduction is a vital surgical option for treating Developmental Dysplasia of the Hip, especially in cases where non-surgical methods are inadequate. With careful patient selection, meticulous surgical technique, and appropriate postoperative care, open reduction can restore hip anatomy and function, preventing long-term disability.
Early diagnosis and timely intervention remain the cornerstone of successful DDH management. Parents and caregivers should seek prompt medical evaluation if hip instability is suspected in infants to optimize outcomes.
Aenean porta orci nam commodo felis hac ridiculus fusce fames maximus erat sed dictumst blandit arcu suspendisse sollicitudin luctus in nec