Blount’s disease is a growth disorder affecting the tibia (shin bone), leading to progressive bowing of the lower leg. This condition primarily affects children and adolescents and can cause significant deformity, gait abnormalities, and functional impairment if left untreated. Correcting Blount’s disease is essential to restore normal leg alignment, improve mobility, and prevent long-term complications such as arthritis.
In this article, we provide an in-depth overview of Blount’s disease correction, including its causes, diagnosis, treatment options, surgical techniques, and postoperative care.
Blount’s disease, also known as tibia vara, is a growth disorder of the medial (inner) part of the proximal tibial growth plate. This abnormality causes the tibia to grow unevenly, resulting in a varus deformity — where the lower leg angles inward, creating a bowleg appearance.
The disease is classified into two main types based on the age of onset:
The exact cause of Blount’s disease is not fully understood, but it is believed to involve a combination of genetic, mechanical, and environmental factors. Excessive weight and early walking may increase stress on the growth plate, contributing to the development of the deformity.
Children with Blount’s disease typically present with:
Early diagnosis is crucial to prevent permanent deformity and joint damage.
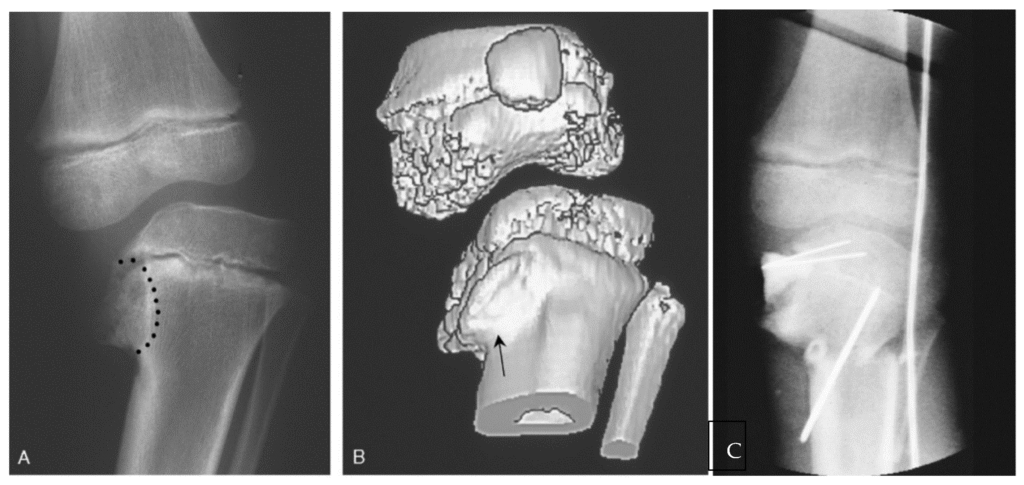
Diagnosis of Blount’s disease involves a combination of clinical examination and imaging studies:
The goal of treatment is to correct the varus deformity, restore normal mechanical alignment, and prevent progression. Treatment depends on the patient’s age, severity of deformity, and stage of disease.
Non-surgical management is generally reserved for very young children (under 3 years) with mild deformity. This includes:
However, bracing has limited success in more advanced or older cases and is not effective once the deformity has progressed.
Surgery is the mainstay of treatment for moderate to severe Blount’s disease or when non-surgical methods fail. The choice of surgical technique depends on the patient’s age, deformity severity, and growth potential.
This is the most common surgical procedure for Blount’s disease correction. It involves cutting the tibia near the knee and realigning it to correct the varus deformity.
Types of Osteotomy:
Fixation: Internal fixation with plates and screws or external fixation devices stabilizes the osteotomy site.
Advantages: Immediate correction of deformity, reliable results.
Considerations: Requires careful preoperative planning to avoid over- or under-correction.
For younger children with remaining growth potential, guided growth is a minimally invasive option.
In complex or severe deformities, external fixation devices such as the Ilizarov frame or Taylor Spatial Frame may be used.
Successful correction requires detailed preoperative planning:
After surgery, proper care is essential for optimal outcomes:
While surgical correction is generally successful, complications can occur:
Early detection and management of complications improve outcomes.
With timely and appropriate treatment, most children with Blount’s disease achieve good functional and cosmetic results. Untreated or late-treated cases may develop:
Therefore, early diagnosis and intervention are critical.
Blount’s disease correction is a complex but manageable condition with a variety of treatment options tailored to the patient’s age and deformity severity. Early recognition and intervention, whether through bracing, guided growth, or surgical osteotomy, can restore normal leg alignment and function, preventing long-term disability.
If you or your child has been diagnosed with Blount’s disease, consulting an experienced orthopedic specialist is essential to determine the best treatment plan. Advances in surgical techniques and postoperative care continue to improve outcomes for patients with this challenging condition.
Aenean porta orci nam commodo felis hac ridiculus fusce fames maximus erat sed dictumst blandit arcu suspendisse sollicitudin luctus in nec